
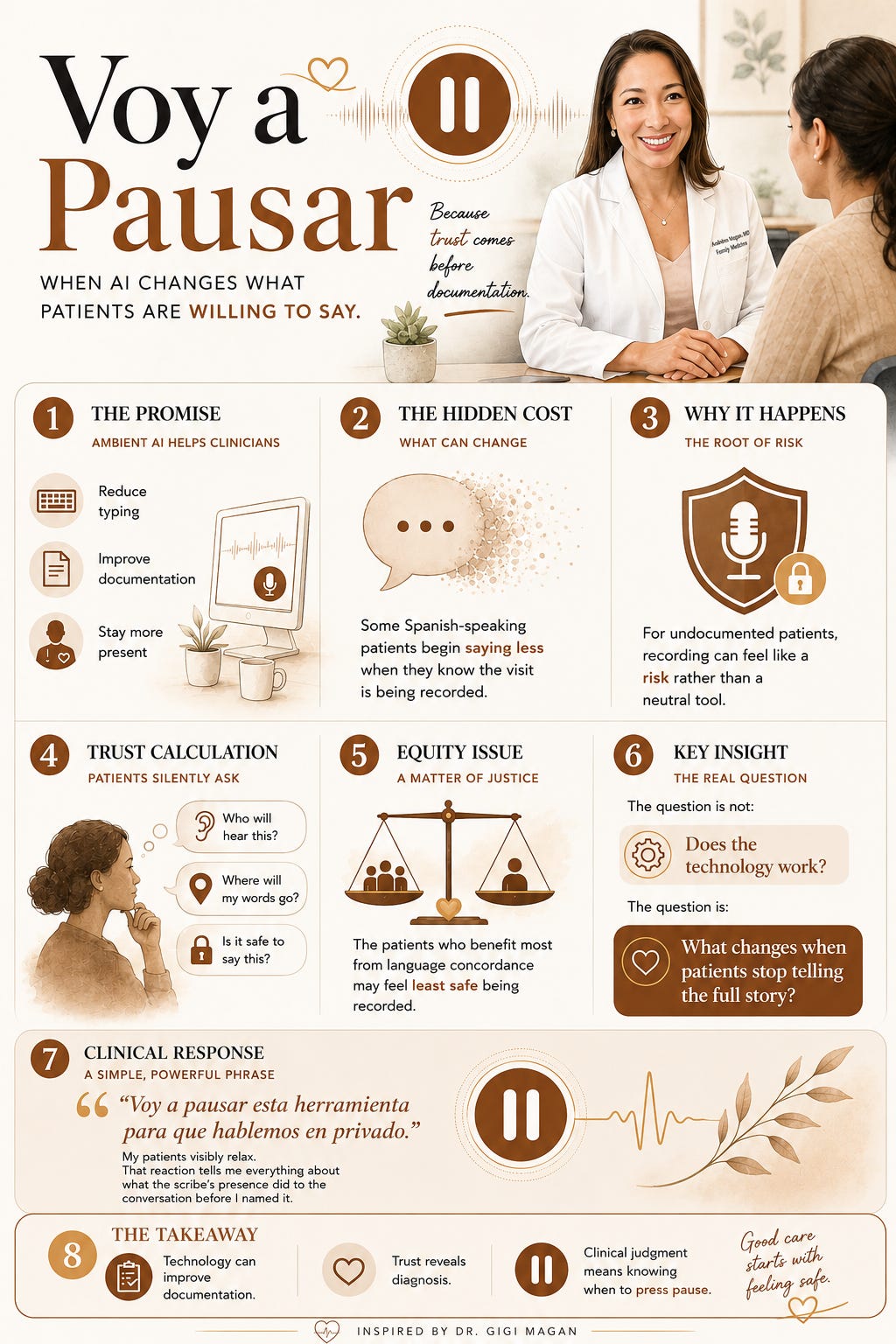
Voy a Pausar
What ambient AI changes in language-concordant safety-net visits, and the deliberate move I now make in the exam room.

I see it in my own exam room, not in a meeting. A patient I have known for a few months pauses before answering my question about her living situation. She normally tells me everything in Spanish. Not today. She glances at the computer. She shortens her answer. She moves on.
I have seen this before. Not once. A pattern.
Later, in a team meeting, a colleague on our language-concordant care group describes the same thing. She does not use the ambient AI scribe as much as the rest of us. Not because it failed. Because her patients stopped talking the way they used to. She frames it as a trust calculation her patients make in real time.
I keep coming back to that phrase. Trust calculation. The kind that happens in the half-second between question and answer, before the words come out. The kind I do not see on any vendor demo.
What the Recording Changed
Language concordance is one of the most effective tools in primary care. When I speak to a patient in Spanish, without an interpreter, the clinical encounter changes. More information surfaces. More context. More truth. It is how I was trained. It is what my patients deserve.
Ambient AI scribes are designed to capture that encounter. I use one in roughly 80% of my visits. It reduces cognitive load. It keeps me present with the patient instead of buried in the note. I am not going back to typing everything by hand.
For some of my patients, though, the presence of recording technology reverses what language concordance was supposed to give them.
When a patient is undocumented, speaking in Spanish about details that touch immigration status or housing conditions, a recording device is not neutral. It is a risk variable. And I watch it happen in real time: the sentence that gets shorter, the detail that gets left out, the pause before answering.
The political climate matters here. In 2026, the question is not hypothetical. My patients are making decisions about what to disclose based on where they believe their words will go.
Where Risk Shows Up First
In my exam room. In the language-concordant visit. In the safety-net clinic where patients already know that systems built to help them have sometimes been used against them.
A colleague raised the data storage question. The audio is held for 30 days. What happens after that? Who has access during those 30 days? If a subpoena comes, what is protected? Is it possible to request a shorter retention window?
These are not paranoid questions. They are informed ones. And the answers are not as clear as the consent form implies.
Speech recognition models carry systematic bias, with higher error rates for non-native English speakers. I see this in my own notes. The tool is least accurate for the patients most cautious about being recorded. The gap between what my patient says in Spanish and what the tool captures widens where it matters most.
Why This Creates Ethical Tension
The value proposition of ambient AI is direct: better documentation, less typing, more eye contact. Those gains are real. I experience them daily.
The value proposition assumes a patient willing to speak freely. For a meaningful number of my patients, that assumption does not hold.
The technology is doing what it was built to do. The clinic is where the harm shows up. Implementation context is the variable, not the technology. The same tool that works well in a suburban dermatology practice risks creating harm in a community health center serving predominantly immigrant patients. Not because the tool is different. Because the room is different. I work in both kinds of rooms. I see the difference.
Equity Lens
The patients who benefit most from language concordance are often the patients who carry the most risk from ambient recording. That is not a coincidence. It is a structural pattern. And I live inside that pattern every clinic day.
When we implement ambient AI without accounting for this, we ask the technology to serve a population it was not designed to understand. The consent process is in English. The FAQ is on a website. The opt-out requires the patient to interrupt her own visit to make a request.
None of that is designed for the patient who is already managing fear about what happens when institutions collect her information. I know these patients by name. I have built trust with them over years. And I watch a recording device complicate that trust in seconds.
Research evaluating ambient AI scribes specifically within FQHCs, rural clinics, and non-English speaking populations is missing. We are implementing first and studying later. In safety-net settings, that order matters.
How I Now Think About This
Ambient AI should not be removed from safety-net settings. Removing it would leave clinicians in under-resourced systems without the tools well-resourced systems already use. The shift for me is not whether to use the scribe. It is when.
I now pause it deliberately before any conversation that touches immigration status, housing, intimate partner violence, or undocumented family members. Anything my patient would not say if she thought someone outside the room might read it.
Implementation in these settings needs to be different. Consent needs to be multimodal, multilingual, and offered as a genuine choice, not a buried clause. Clinicians need training on when to pause the tool, not only how to use it. And institutions need to be honest about what they do not yet know about long-term effects on patient disclosure.
I say it in Spanish: “Voy a pausar esta herramienta para que hablemos en privado.”
My patients visibly relax. That reaction tells me everything about what the scribe’s presence did to the conversation before I named it.
My colleague did not reduce her use of the scribe because she dislikes technology. She scaled back because she noticed her patients holding back. She decided what they were holding back was more important than what the scribe was capturing.
That is clinical judgment in action. The kind no AI replicates.
Digital Health Pearls
Language concordance is clinical infrastructure. Ambient recording undermines it.
Data retention timelines matter less than data access pathways. Ask who sees it, not how long it is stored.
The consent form is not the same as informed consent. Informed means the patient understood and still chose.
Implementation context is not a footnote. It is the variable that determines whether a tool helps or harms.
TL;DR
Ambient AI works differently in different rooms. I work in the rooms where it gets complicated.
Language-concordant visits with undocumented patients carry specific risks that vendor demos do not model.
Your colleagues who scaled back the scribe are not behind. They are paying attention.
Ask your institution: what is the consent process for patients who are afraid of recording? If the answer is the same process as everyone else, it is not enough.
Invitation to Compare Notes
Has your institution differentiated its ambient AI consent process for patients with specific risks from disclosure? Do you pause the scribe in language-concordant visits? What would it take for your clinic to have this conversation honestly?
Disclaimers: All views expressed are my own and do not represent my employer or any institution I am affiliated with. Any tools, products, or technologies mentioned are included for educational purposes only and are not sponsored or endorsed. Nothing in this piece should be interpreted as medical advice.
Hi Doctor! Thanks for sharing your insight and expertise on this matter. Are you aware of any issues in regards to NLP and difficulties with transcribing the voices of patients who may speak with an accent?